Interventional Radiology Newsletter
Welcome to the first Aquilant Interventional Radiology Newsletter! Keep up-to-date with the latest technology and innovation across GI Intervention, Oncology and Vascular therapy. Explore insightful case reports from leading clinicians across the UK.
BSIR 2024 – 6th – 8th November 2024
We are excited to be supporting this year’s BSIR Annual Scientific Meeting at The Brighton Centre. This meeting provides fantastic learning opportunities for anyone with an interest in vascular and non-vascular, with sessions hosted by national and international speakers it has proven to be a highlight in the Interventional Radiology calendar.
The Active Learning Zone is a pivotal part of the meeting and we are pleased to be supporting these sessions with our AngioDynamics NanoKnife IRE and Solero ablation systems as well as the TaeWoong GI and HPB stents.
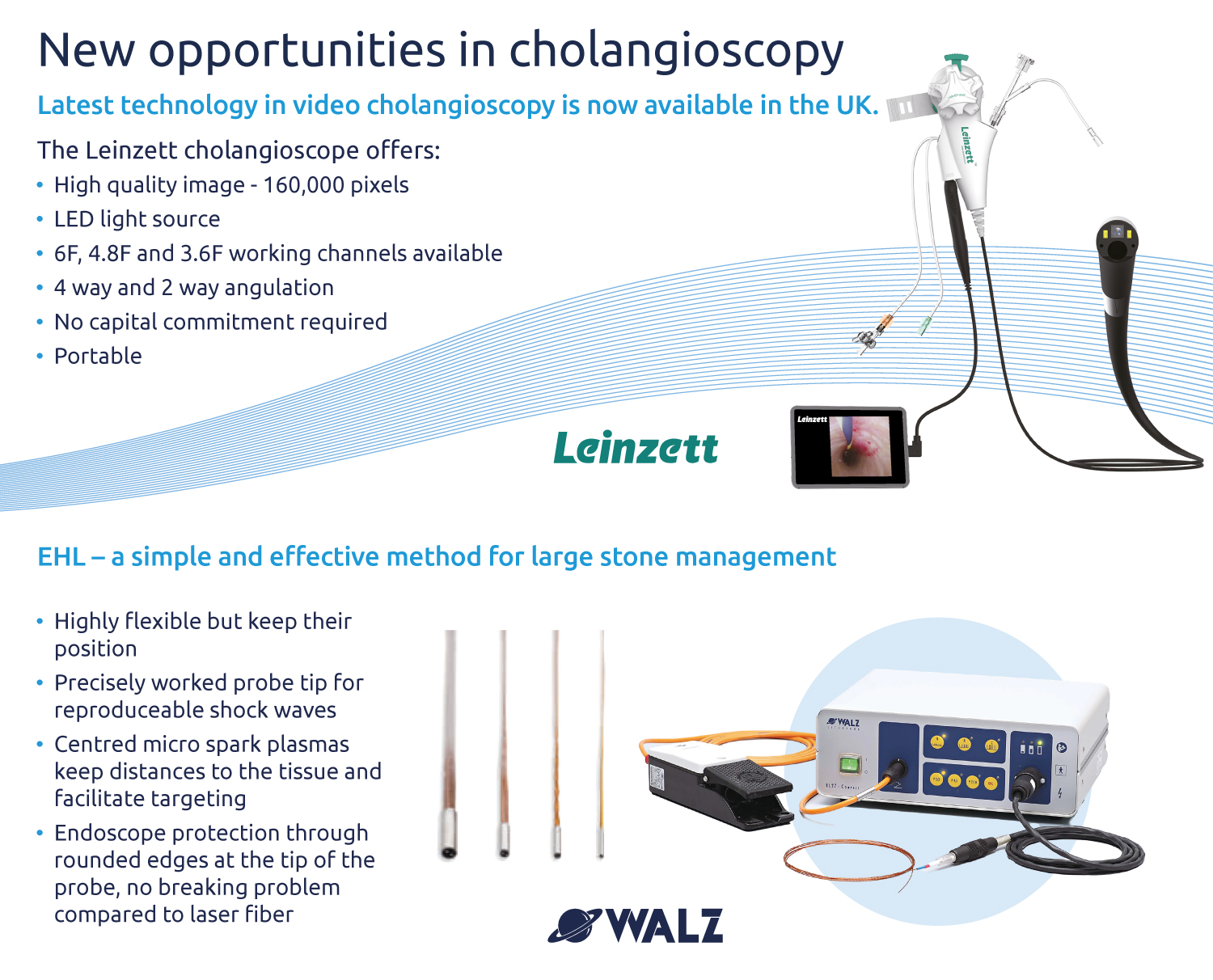
Please make sure you visit the Aquilant stand in the exhibition hall! There will be the latest technology in the Interventional Radiology world including the new AngioDynamics Auryon Atherectomy System, Leinzett portable video cholangioscope, NanoKnife IRE system, Balt embolisation portfolio as well as the latest offering from Cardionovum, Optimed and TaeWoong.


We welcome Auryon to the Aquilant family!
The Auryon Atherectomy system from AngioDynamics recently celebrated its 4th birthday in the Americas’ with almost 100,000 cases completed in that time. Following this success, we are delighted to announce that as of 2nd September 2024, Auryon has received its CE mark and is now fully available for use in the UK.
More than just another Atherectomy system:
The Auryon Atherectomy system is a 355nm Laser that has the capability to break through calcium, aspirate clot and deliver lithotripsy effects (as demonstrated in the Micro CT study) to address medial arterial calcification. In addition, the 2.0 and 2.35mm fibres are indicated for in stent restenosis. It’s clear that Auryon is not just another atherectomy device but more of a vessel preparation system that is tailored to assist our doctors in treating some of their more complex patients.
Indications:
Auryon is indicated to treat Peripheral Arterial Disease below the level of the inguinal ligament and In Stent Restenosis* (ISR).
Key Benefits:
- Clear all lesion types, including ISR*, with one single device.
- Revolutionize how you treat, above and below the knee.
- Practice with confidence by minimising the risk of embolisation.
*Only the 2.0 & 2.35mm catheters are indicated for ISR.
If you are attending the BSIR meeting, please visit the Aquilant stand for a demonstration.

Treatment of a distal malignant oesophageal stricture using a Niti-S covered oesophageal stent
Introduction:
At Guy’s and St Thomas’ NHS Foundation Trust we use the Niti-S Oesophageal stent as part of our tool kit in treating oesophageal malignancy. This double layered covered stent and its anti-migration technology allows us to treat a range of oesophageal strictures confidently.
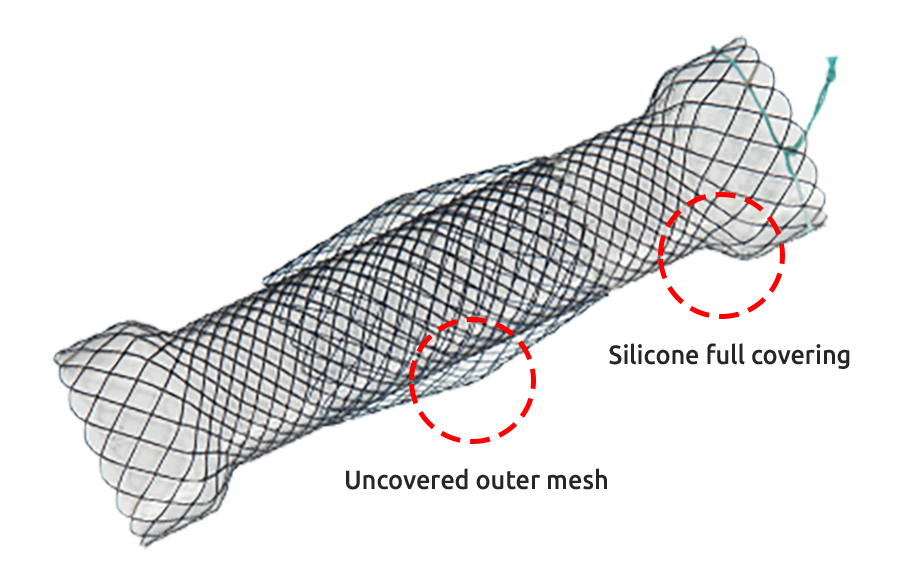
Image 1
Indications:
The Niti-S oesophageal Stent (Image 1) is intended for use in oesophageal strictures caused by intrinsic and/or extrinsic malignant tumours.
Key features:
- The stent has a fixed cell with braided construction offering high flexibility and optimal radial force.
- Proximal and distal head ends (8mm larger than trunk) to minimize migration
- Double-layered design: an inner polyurethane layer to prevent tumour ingrowth and an outer uncovered nitinol wire tube to allow the mesh of the stent to embed itself in the oesophageal wall.
- 10 radiopaque markers in three locations –four proximal, two middle and four distal – allowing for accurate deployment and ensuring adequate lesion coverage.
Case presentation:
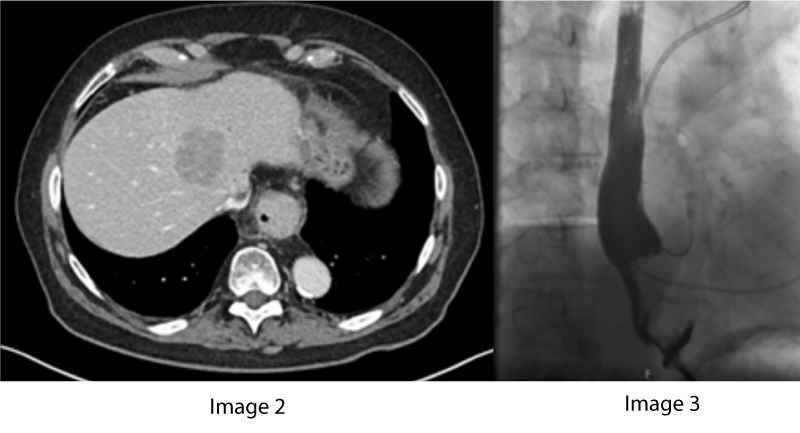
A 77-year-old gentleman presented with progressive dysphagia. This was on a background history of Barrett’s oesophagus and ischaemic heart disease. A contrast enhanced CT of the thorax, abdomen and pelvis revealed a 6 cm obstructing distal oesophageal mass lesion extending to the gastro-oesophageal junction (GOJ) with hepatic metastases (Image 2). A fine needle aspirate from oesophagogastroduodenoscopy (OGD) yielded a diagnosis of moderately differentiated adenocarcinoma with a provisional staging of T3N1M1.
He commenced palliative chemotherapy with a mixed response, but represented with progression of the primary lesion causing obstructive symptoms. A contrast swallow study revealed high grade stenosis of the distal oesophagus at the level of the known mass lesion (Image 3).
Procedure:
The patient was referred to interventional radiology for oesophageal stenting. The case was performed under general anaesthetic with transoral cannulation of the stomach and placement of a guidewire in the duodenum.
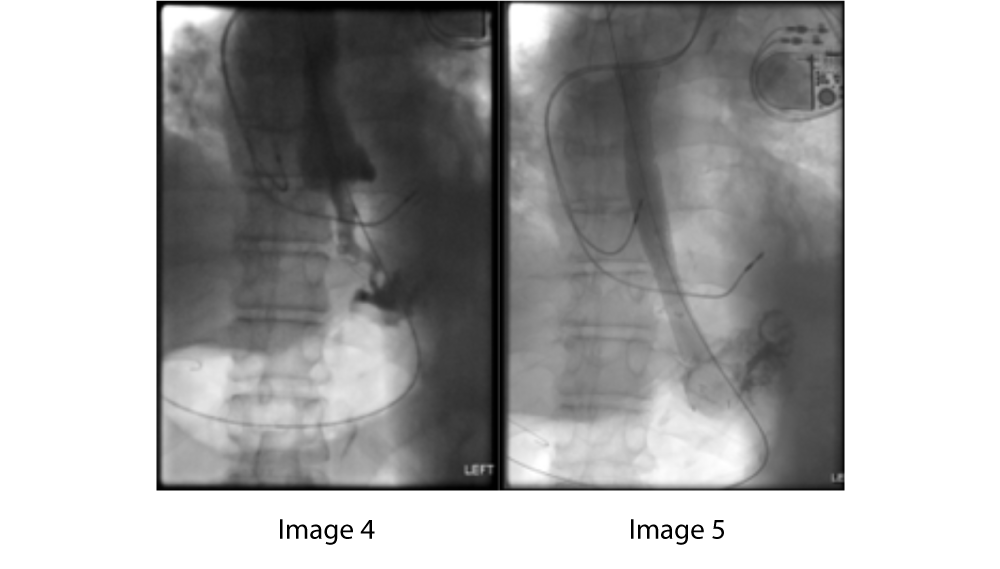
A 5 french long sheath was inserted, through which a pullback oesophagogram was performed to identified the lesion and plan stent size, and placement (Image 4).
An 18 french 18 mm x 120 mm covered stent was loaded over the wire and advanced to the distal oesophagus where it was deployed without complication (Image 5).
Balloon dilatation was performed in the midportion of the stent, at the site of known malignant stenosis.
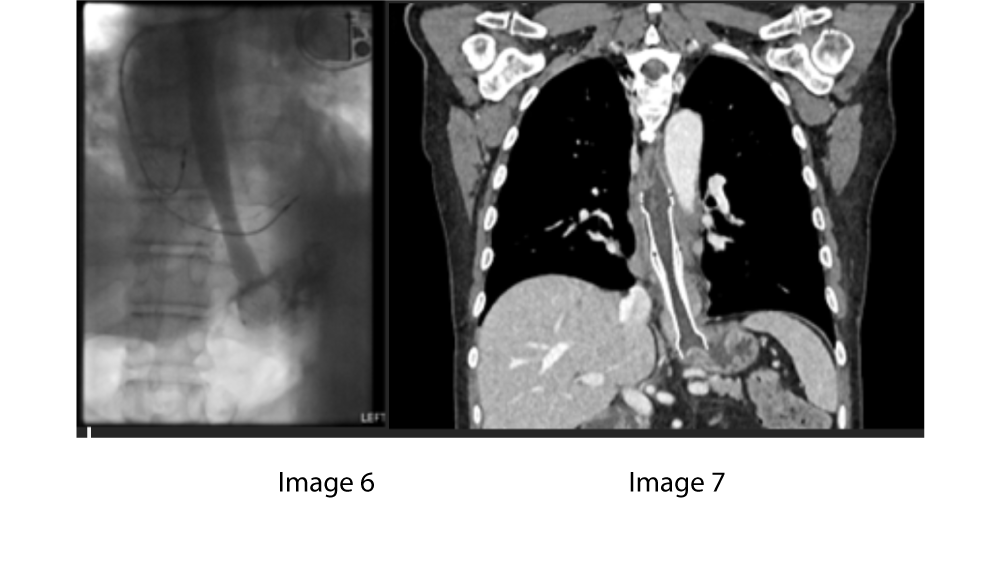
An oesophagogram performed thereafter demonstrated appropriate positioning and patency of the stent (Image 6).
Two months later a follow-up CT demonstrates that the stent remains widely patent and well positioned (Image 7). The features minimising stent migration; the double layer, along with the proximal and distal end heads of the stent, can be well seen on this CT.

Dr Olly Hulson discusses focal therapy and how NanoKnife is an innovative treatment solution for treating patients with prostate cancer.
Thank you to Dr Olly Hulson (Consultant Radiologist) from Leeds Teaching Hospitals NHS Trust for discussing his thoughts around focal therapy and the benefits of using the NanoKnife system on patients with intermediate-risk prostate cancer.
The NanoKnife IRE system from AngioDynamics enables clinicians to confidently treat all segments of the prostate, effectively destroy targeted tissue delivering precise treatment margins and preserve vital structures inside the ablation zone including nerves.
What do Interventional Radiologists have to say about the sought after liquid embolic peripheral embolisation course in Dijon?
The liquid embolic peripheral embolisation one and a half days workshop in Dijon is held 5 times throughout the year (January / April / July / October / December) The July course is dedicated for UK Consultants only.
The program is intended to provide physicians with a broad understanding of advanced techniques using liquid embolic agents where participants will review the embolisation techniques with the use of Squid Peri, Magic Glue & Prestige detachable coils.
Professor Romaric Loffroy leads this interactive workshop from the Francois Mitterrand University hospital in Dijon (a short tram trip from the hotel).
Participants’ can enjoy a mixture of lectures on liquid embolic agents for peripheral use, tips & tricks & live patient cases where consultants can have practical & technical use of the liquid embolic agents (squid peri & magic glue)
A maximum of 8 participants per workshop allows enough time on live cases and clinical discussion.
This is a popular course and many consultants who have attended over the years have found it to be both informative and insightful.